

With global development institutions in retreat, it is becoming more and more obvious that the public sector is unambiguously the primary enabler of ‘global’ development—capable of propelling development forward by embracing inclusive and effective multilevel governance systems—and equally capable of bringing progress to a halt if it doesn’t.
Multilevel governance systems as a catalyst for inclusive and sustainable development
To many members of the Local Public Sector Alliance, it is clear that inclusive and efficient multilevel governance systems can—and should—be leveraged to contribute to global stability, economic prosperity, and efficient public services in countries around the world.
Regardless of the subnational structure of a country’s public sector, ensuring responsive public services will require dedicating an adequate share of public resources to frontline services (i.e., an efficient vertical allocation of resources); public sector resources will need to be distributed efficiently, equitably, and transparently across the national territory (i.e., horizontal allocation of resources); and public sector resources need to be efficiently transformed from public sector inputs (e.g., public finances and human resources) into public sector outputs and outcomes (e.g., impactful public services and infrastructure) at the local level.
While all of this sounds good in theory, one might ask: is it possible to quantity the potential benefit of more effective multilevel governance in practice?
In fact, yes, we can. A simple exercise with real-world data can show that the potential benefit of effective localization of public service delivery has the potential to create much greater value-for-money than is the case under a ‘business as usual’ scenario. A back-of-the-napkin analysis of health spending in India reveals that the potential efficiency gain of effective decentralized governance of primary health service in India could be as much as 46 billion dollars per year.
The value of effective decentralized governance and services: the example of primary health spending in India
Under India’s decentralized approach to health care delivery, state governments are primarily responsible for organizing and delivering public health services. However, as a federal country, some Indian states are more effective than others at leveraging local government institutions to ensure better health services and better health outcomes.
As an aside, the Amazon series Gram Chikitsalay (Village Health Center) –albeit humorous fiction—does a great job highlighting some of the real world challenges of rural health care in many parts of India.
Perhaps the most obvious single indicator of the public sector’s performance in the provision of public health services is the number of people that seek—and are provided with—healthcare services at public health facilities. When access to—or the quality of—public health services is poor (or if the health provider does not show up), the number of patients that receive outpatient health services should be expected to be smaller. When access to—or the quality of—public health services is better (when the health provider shows up on a regular basis, and when the public sector provides medical supplies to frontline facilities in adequate quantities), the number of patients that show up for outpatient health services is generally greater. As such, the number of people that receive primary healthcare services (measured as the number of public health facility ‘outpatients’ per thousand residents) is a pretty good indicator for the quantity and quality of public health services provided.
In this case, the “value for money” that the public sector provides to taxpayers by providing primary healthcare services can simply be defined as public health spending divided by the number of outpatients serviced by public health facilities. In other words, what is the cost to the public sector per outpatient?
In India, for the most recent year for which data are available (2021/22), public primary health facilities provided services to 1.43 billion patients, at a total cost of approximately 1.67 trillion Rupees (or 1.67 lakh crore rupees), equivalent to 19.2 billion US dollars.[1] This means that, on average, Indian citizens make roughly one outpatient visit to a public health facility per year, and that they—through the public sector budget—spend approximately 1,170 rupees (or roughly 13 US dollars) per outpatient primary healthcare visit, inclusive of related expenses (such as labs).
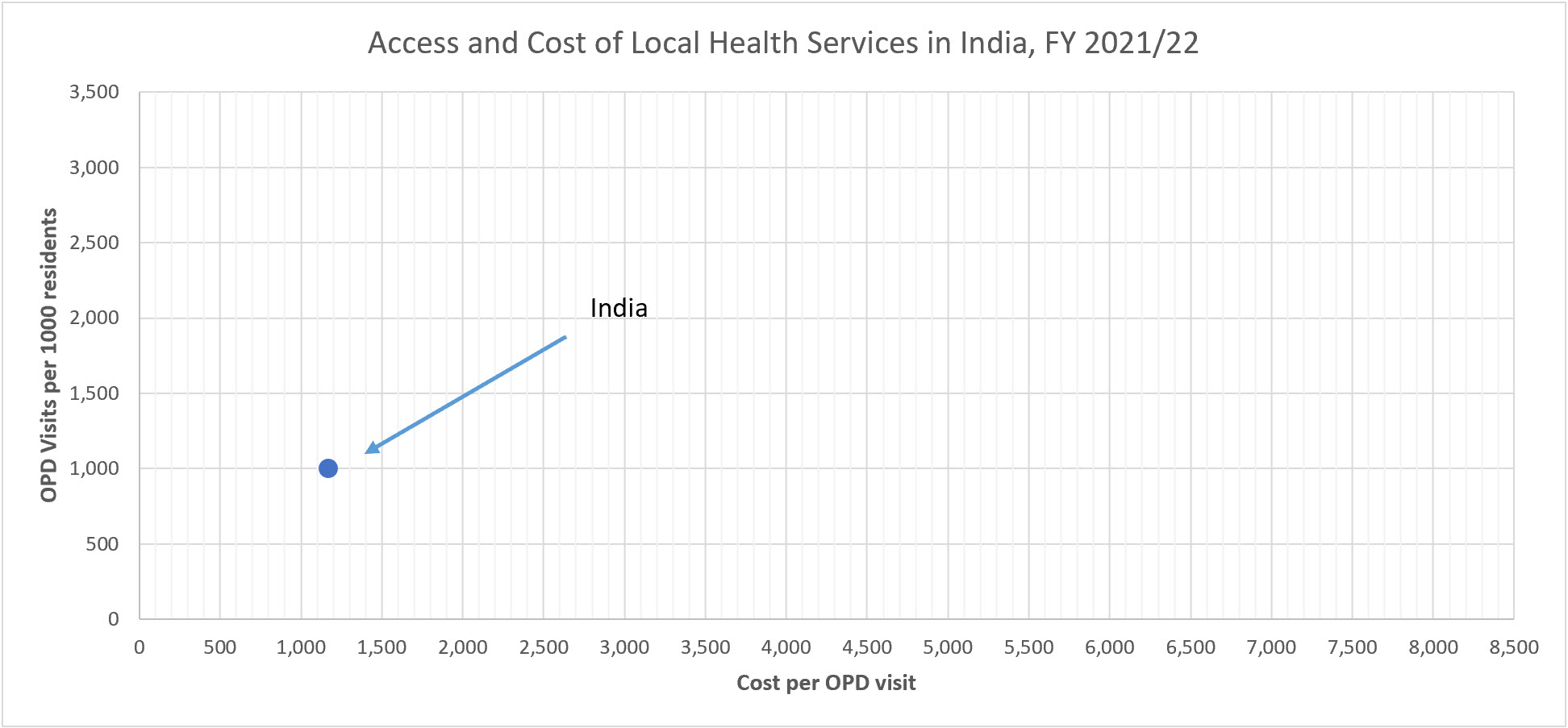
This single data point tells us very little about the performance of India’s public sector when it comes to primary healthcare services, other than that the number of public healthcare visits seems to be on the lower end of the international spectrum. In reality, because of severe shortages of staff and supplies at government facilities, many households seek care from private providers and pay out-of-pocket. Yet, total national figures do not provide any insight into why public provision of health services is low, or how to improve the performance of primary health services. The conventional wisdom on how to improve health services in the world (or achieve sustainable development) does not focus on results or value-for-money: it simply suggests that more public spending is needed to achieve ‘better results’.
A disaggregated analysis of primary healthcare access and cost-per-patient
A disaggregated analysis, however, provides much greater insight into the sector than a single national performance data point. What if we were to consider primary health expenditures in India at the state or local level?
While it would be highly desirable to consider primary healthcare access and cost-per-patient at the district level (or below), neither national governments nor state data sources readily break down health results or health spending at the district level in India. However, relevant state-level data is available.
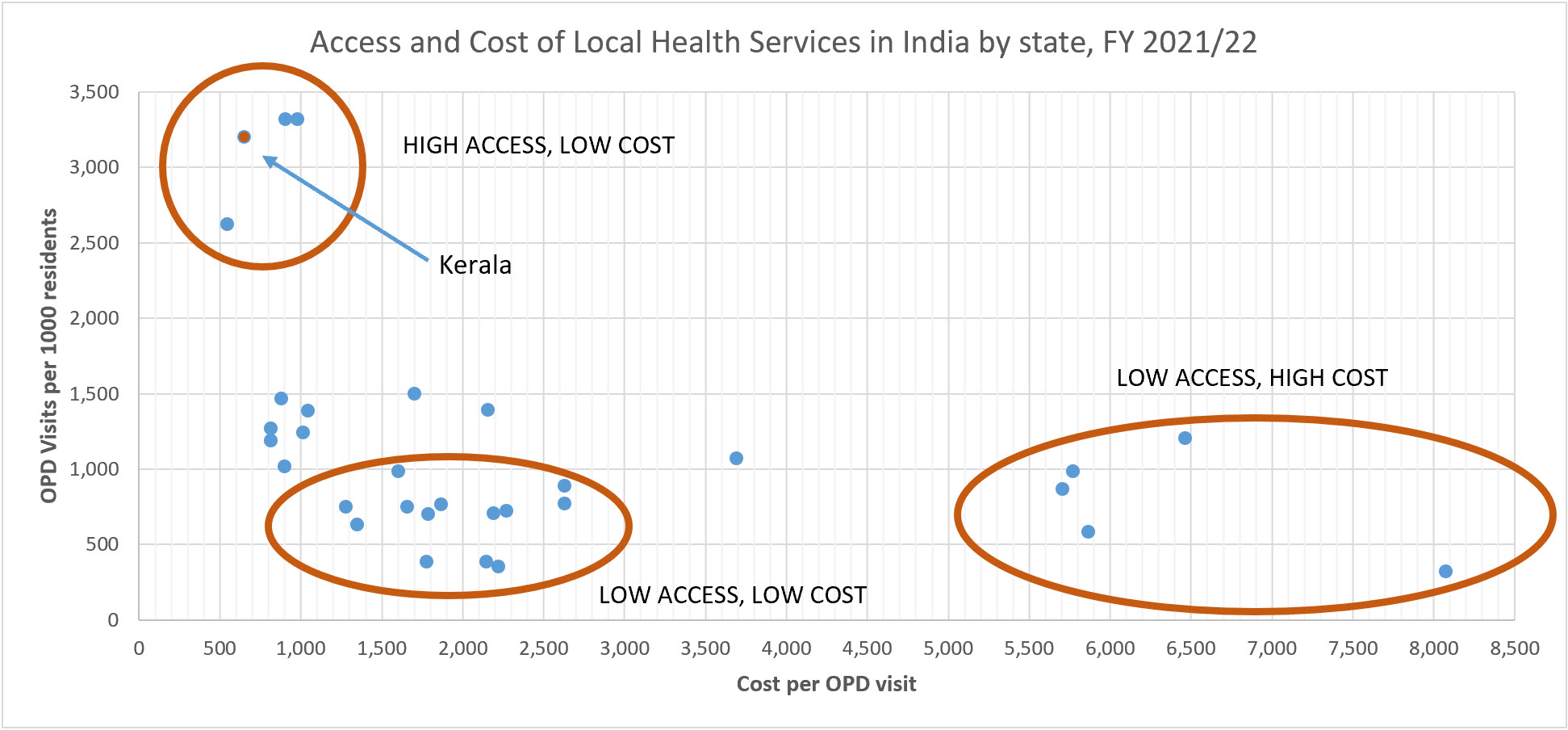
Using data from the Ministry of Health and Family Welfare (on outpatient attendances by state) and the Reserve Bank of India (on state government spending by function), the graph below shows the level of access to primary healthcare services at the state-level in India, revealing considerable variation in the level of healthcare access, as well as in the cost-per-patient or value-for-money being produced by the public sector in different states.
Before looking at the results (below), it is important to recognize that we should not expect access and cost to be exactly the same across a country’s national territory. Given that primary health services are to be delivered in the cities, towns, and rural communities where people live and work, we would expect access to primary healthcare services and per-patient costs to vary based on a range of factors, including variations in geographic, demographic, social, and economic conditions.
Click here to view an interactive version of the chart:
The basic subnational analysis of health spending and access in India reveals that some states are ‘high access, low-cost’ states when it comes to primary health services, while other states are ‘low access-low cost’. Then there are ‘low access-high cost’ states.
The states that provide greater access to health services at lower cost are the ones to learn from. For instance, in Kerala—one of the most decentralized states in India—on average, people seek healthcare at public health facilities at the rate of 3,195 per 1000 residents, which is three times higher than the national average. At the same time, the average cost per outpatient visit in Kerala is 655 rupees, which is half of the national average.
The Fifteen Finance Commission (2020: 213-214) singled out Kerala as a state that “has established itself as an example where local governments and the staff of public health institutions effectively deliver healthcare at the local level in a collaborative framework.” The Commission report further noted the need “to involve the third [local government] tier in the health sector and extend additional resources to it to strengthen the primary health system at the grass root level. We believe that the involvement of local governments would also make the health system accountable to the people.”
The value of effective decentralization: better access and cost savings in health services in India
The analysis based on disaggregated subnational spending and outputs, albeit simple, unlocks a transformative perspective when it comes to improving public sector performance and results.
After all, the path to better health outcomes is no longer simply ‘spending more’, but rather, the multilevel governance perspective provides encouragement to policy makers and implementers in under-performing states to identify changes that they can make to achieve the same results (both in terms of greater access and better value-for-money) as the better-performing jurisdictions.
Of course, some of the variations in access and costs may be caused by exogenous factors that cannot be changed–or may be hard to change–such as low population density or the social-economic composition of the population. But other drivers of the variations in access and costs can be influenced by policy choices. It is those policy choices and implementation reforms that need to be explored, with a view to improving public sector outcomes.
While the impact of more inclusive and accountable subnational governance on service delivery outputs and outcomes takes time, and while it may be hard to induce public participation and public accountability where it does not organically exists, the example of Kerala suggests that there is considerable merit on focusing on public sector performance below the national level, and trying to isolate the impact of more responsive and accountable local service delivery practices to improve the effectiveness of the public sector.
In fact, the subnational analysis of health spending and results in India above allows us to quantitatively compare two scenarios: first, how much would India need to spend in order to achieve the same level of health care access as Kerela using the business-as-usual (‘spending more’) strategy? And second, how much would India need to spend in order to achieve the same level of health care access as Kerela if different states would be able to leverage inclusive and accountable multilevel governance systems to improve the efficiency of public health services?
Under the business-as-usual approach, which would not change the cost-per-patient of delivering primary health services in each state, India would need to quadruple its primary health spending from 1.67 to 6.69 trillion rupees (76.9 billion US dollars) in order to raise access to primary health services from each state’s current level to reach 3,500 outpatient visits per 1000 residents per year.
Achieving that same level of healthcare access across India through improved multilevel governance, public accountability, and citizen engagement—which could potentially reduce the cost-per-outpatient to the same level as in Kerala—would cost much less. The estimated health care expenditures for this scenario equal 2.96 trillion rupees or 34 billion US dollars.
Based on our back-of-the-envelope calculations, the amount of savings to the public sector by leveraging inclusive multilevel governance and effective citizen participation would be 3.73 trillion rupees (or 46.6 billion dollars). In other words, leveraging the lessons from high-performing subnational jurisdictions to deliver better public services—based on a process sometimes referred to as yardstick federalism— could result in primary healthcare services being delivered in a more accountable way across India, resulting in cost savings of literally trillions of rupees (or billions of dollars).
Concluding thoughts
The analysis here aims to convey a simple point: there is no such thing as ‘global development’ or even ‘national development’. Instead, public service delivery and development take place in a spatially localized manner, and the performance of the public sector varies across space. Thus, if you want to improve the performance of the public sector, it is essential to start by considering the delivery of public services and the value-for-money produced by the public sector in a spatially disaggregated manner.
The analysis of disaggregated access and costs recognizes that some places do better than others, and that there is considerable long-term value in pursuing inclusive and efficient multilevel governance systems. These systems encourage community engagement to ensure that public health workers show up to their posts every day, and that they are resourced to perform their jobs well. In turn, this allows citizens to receive quality health services from the public sector in Kerala and a handful of other states, which is not necessarily a given elsewhere in India.
Finally, the analysis shows that—if it would be possible to replicate the benefits of the more inclusive multilevel governance systems and more effective local accountability found in Kerala—the amount of savings to the public sector would be immense. In our example, doing so could save 46.6 billion dollars annually in one sector, in one country.
Admittedly, the example highlights an important sector in a big country. The same principle, however, applies to all sectors and all countries. Achieving an effective, high-performing public sector is not easy. But it starts by shifting the les from the national level to the subnational level, and recognizing that all development and all public services are local.
This blog was authored by Jamie Boex, and first published on Decentralization.Net on August 18, 2025. Jamie is LPSA’s Executive Director. This blog reflects the author’s own analyses and opinions.
The analysis in this blog relies in part on background analysis prepared by Dr. Boex for the World Bank report: Reviewing India’s XVFC Local Health Grants through a comparative global lens: Observations and recommendations for the 16th Finance Commission.
[1] This analysis assumes that each Indian state spends 60 percent of its state health expenditures on primary health services, as opposed to hospital services, health administration, and other public health services.



